

This is generalised inflammation of the faucial tonsils and is usually caused by haemolytic streptococci. It can occur at any age, but more common in children and adolescents.
Pathological types
1. Acute parenchymatous type - where tonsils are inflamed and enlarged.
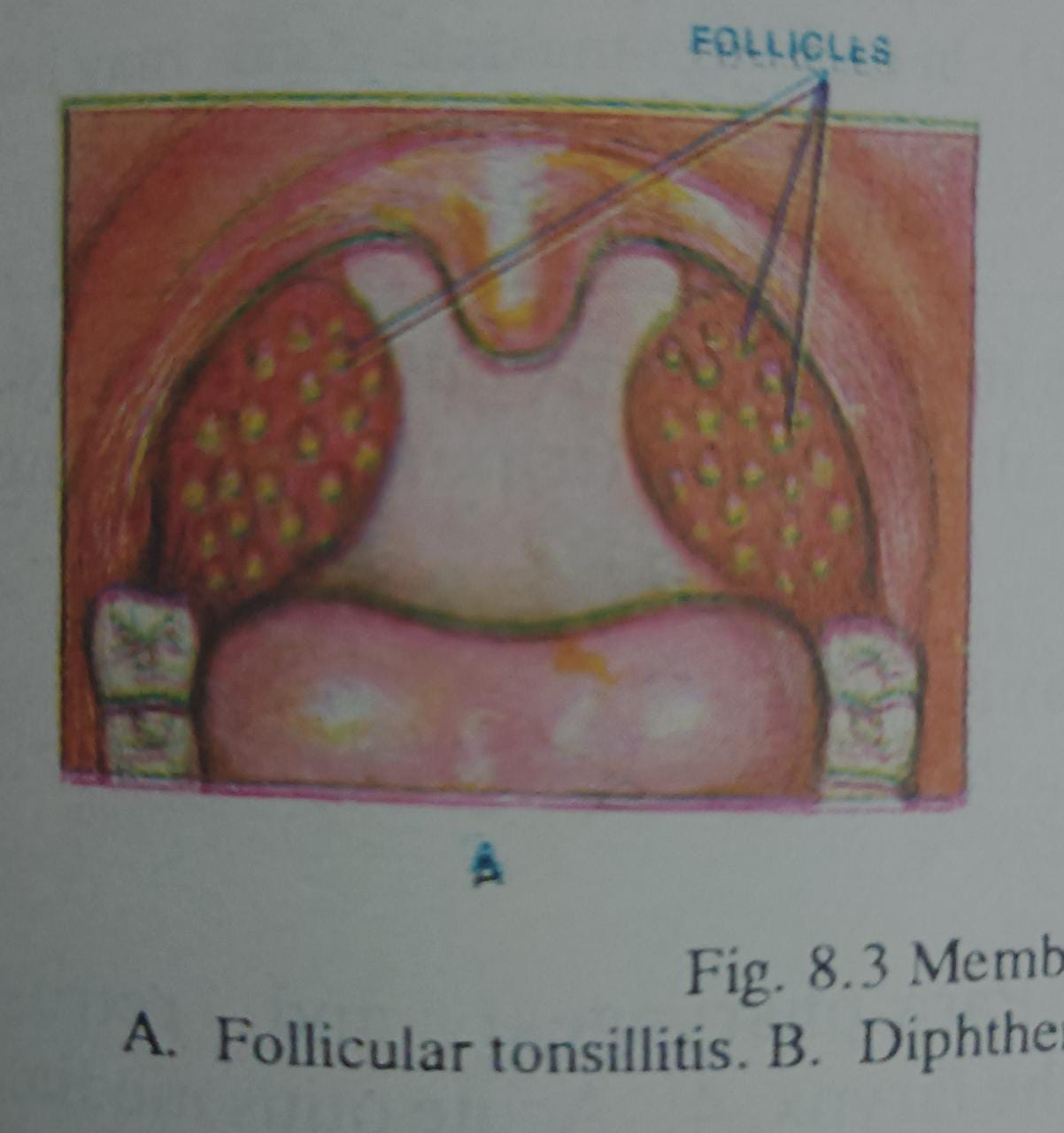
2. Acute follicular type - where tonsils are inflamed with multiple follicles on its medial surface.
Clinical features
Symptoms
1- Sore throat is the commonest complaint. Younger children do not complain of much sore throat, but refuse to eat food.
2- There is high rise of temperature, difficulty in swallowing, and pain on swallowing.
3- Associated features are malaise, headache and constipation. Earache is quite common. Patients usually take to bed and children go off school.
Signs
1- The temperature is often 103-104 ° F. and the child is flushed.
2- The tonsils are enlarged and congested. In cases of follicular variety, the tonsils are studded with yellowish spots over the crypts. The follicles often coalesce forming patch on tonsils.
3- The surrounding area of the pharynx is often inflamed. Tongue is furred and breath of foetid.
4- The tonsillar lymph nodes are enlarged and tender on both sides.
Acute follicular tonsillitis
1. Can occur at any age, but more common in children above 5 years and adolescents.
2. Onset – acute.
3. Temperature high (103 104 " F)
4. Constitutional symptoms – more.
5. Dysphagia and sore throat – more.
6. Toxic features – less.
7. Tonsils are enlarged and acutely congested.
8. Patch on tonsils (Pseudo membrane) (a) Multiple follicles, some may coalesce resembling patch (b) Bilateral (c) Limited on tonsils. (d) Yellowish, creamy colour. (e) Thin and superficial. (f) Easily removable with swab. (g) No bleeding on removal.
9. Swab from patch - B Haemolytic streptococci.
10. Enlarged tender tonsillar gland, usually bilateral.
Complications and sequelae
1. Peritonsillar abscess.
2. Para - pharyngeal and retro pharyngeal abscess.
3. Oedema of the larynx.
4. Acute otitis media.
5. Septicaemia.
6. Acute rheumatism.
7. Acute nephritis.
Management
1- Patient is put to bed.
2- Temperature is controlled by giving antipyretic drugs.
CHRONIC TONSILLITIS
This is of two varieties
1. Chronic parenchymatous tonsillitis- seen in children and adolescents.
2. Chronic fibrotic tonsillitis- common in adults. Usually follows acute or subacute recurrent attacks of tonsillitis.
Clinical features
1. There is history of recurrent sore throat, difficulty in swallowing, and rise of temperature. There may be occasional malaise, pain in the limbs, and feverishness. Hawking is common and also choking. Adults often complain of unpleasant taste and smell from cheesy material from the crypts.
2. On examination tonsils are usually enlarged in children and adolescents, but in adult the tonsils are often fibrotic from recurrent attacks. There is flushing of anterior pillars of the tonsils. On pressing the anterior pillars, pus comes out of the tonsillar crypts which indicates persistent tonsillar sepsis.
3. The tonsillar glands are persistently enlarged and tender, located 1/2 inch below and behind the angle of the mandible ( Jugulo - digastric node).
4. In chronic fibrotic variety, occasionally, there may be some follicles over the crypts (chronic follicular type).
Diagnosis
is to be made from physiological hypertrophy in children and keratosis pharyngis in adult (in follicular variety). History is very important in the diagnosis of chronic tonsillitis - i.e . recurrent sore throat, difficulty in swallowing, rise of temperatures (at least 3-4 attacks per year)
TREATMENT AT DR. SOHAN LAL CLINIC
The integrated POLYCLINIC facility offers patients to select their treatment either from the Department of Homeopathy or from the Department of Medicine.
We provide scientific, research-based, and professional services to people across the world, aiming to achieve the highest success rate.
A clinic of national fame with 92 Years of legacy in healthcare. Dr. Sohan Lal Clinic is a state-of-the-art Polyclinic offering integrated healthcare facilities, including online consultation and online medicine delivery. We are an established BRAND- highly trusted for having a high success rate in treatment and being globally affordable.
