

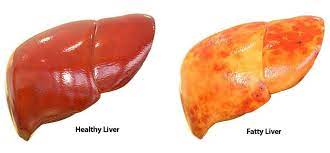
Introduction
• Fatty liver indicates presence of excess fat in the liver.
Causes of Fatty Liver
Alcohol
Non-alcoholic fatty liver disease (NAFLD)
1. Drugs-
• Glucocorticoids
• Amiodarone
• Aspirin
• Tetracyclines
• Methotrexate
• Zidovudine
• Didanosine
• Tamoxifene
• Amiodarone
2. Nutritional
• Protein-calorie malnutrition
• Total parenteral nutrition
• Rapid weight loss/obesity
3. Metabolic
• Lipodystrophy
• Pregnancy (acute fatty Iiver)
• Diabetes
4. Miscellaneous
• Inflammatory bowel disease
• HIV infection
• Reye's syndrome
• Obstructive sleep apnoea
• Indian childhood cirrhosis
• Chronic hepatitis C
Alcoholic Steatosis and Steatohepatitis
• The severity of fatty involvement is roughly proportional to the duration and degree of alcohol intake.
• Most common feature is hepatomegaly with or without tenderness or discomfort.
• Occasionally, patients develop icterus and nausea.
• Many patients may develop cirrhosis of liver with its associated complications.
• Laboratory features include elevated ALT and aspartate aminotransferase (AST) with AST: ALT > 1.
• Ultrasound shows diffuse increase in echogenicity as compared to the kidneys and spleen.
• On CT scan, fatty infiltration produces a low-density liver as compared to spleen.
• Treatment is complete abstinence of alcohol and nutritional support.
Non-Alcoholic Fatty Liver Disease (NAFLD)
• Non-alcoholic fatty liver disease (NAFLD) is classified into two categories: simple fatty liver (non-alcoholic steatosis) with a favourable clinical outcome and non-alcoholic steatohepatitis (NASH), which is intractable and progressive.
• Important risk factors for development of this entity are obesity, type 2 diabetes mellitus, hyperlipidaemia and insulin resistance.
• Non-alcoholic fatty liver is a common cause for abnormal liver tests.
• Most patients have no symptoms at the time of diagnosis, although some have fatigue, malaise and a sensation of fullness in the upper abdomen. Other features may include daytime sleepiness and autonomic disturbances. Hepatomegaly is the only sign in most patients. Many patients are obese.
• Incidence of coronary artery disease increased in patients with NASH.
• Laboratory features include intermittent elevation in ALT and AST with AST: ALT < 1. This ratio increases as fibrosis advances.
• Ferritin levels increased in 20-50% of patients.
• Autoantibodies (e.g. antinuclear and anti-smooth muscle antibodies) identified in nearly 25% of patients and may be associated with more advanced fibrosis.
• Ultrasound and CT features are similar to those in alcoholic fatty liver.
• Liver biopsy remains the best diagnostic tool for confirming fatty liver disease. It is also the most sensitive and specific mean of providing important prognostic information by distinguishing steatosis from NASH and by determining the stage of fibrosis.
• Treatment includes control of weight, diabetes and hyperlipidaemia.
TREATMENT AT DR. SOHAN LAL CLINIC
The integrated POLYCLINIC facility offers patients to select their treatment either from the Department of Homeopathy or from the Department of Medicine.
We provide scientific, research-based, and professional services to people across the world, aiming to achieve the highest success rate.
A clinic of national fame with 92 Years of legacy in healthcare. Dr. Sohan Lal Clinic is a state-of-the-art Polyclinic offering integrated healthcare facilities, including online consultation and online medicine delivery. We are an established BRAND- highly trusted for having a high success rate in treatment and being globally affordable.
